
AI And Predictive Analytics For Clinical Supply Planning
By Shanker Ojha, senior validation lead and operational strategy consultant, Manufacturing Science and Technology (MSAT), Biopharmaceuticals Frameworks, India

The traditional clinical trial supply pipeline is fundamentally broken. Driven by the absolute necessity of preserving patient safety and trial integrity, the industry has historically accepted massive overproduction as a standard cost of doing business. However, when manufacturing a batch of modern monoclonal antibodies (mAbs) or personalized mRNA therapies, a single production cycle features extreme temperature-controlled cold chain dependencies and short expiration horizons.
Table 1 | Comprehensive operational matrix for predictive execution
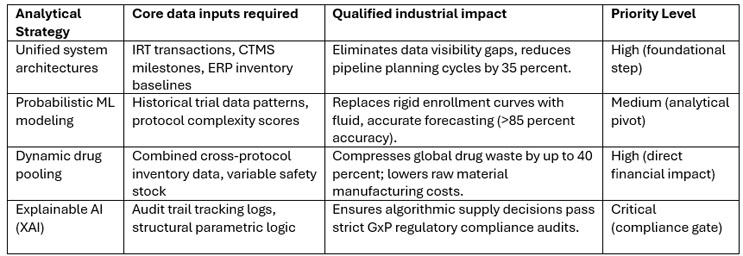
Under these constraints, the legacy strategy of static buffering, where large safety stocks are sent uniformly to all open sites, inevitably leads to high overage rates and extensive product incineration. Conversely, a predictive supply engine utilizes live, multi-stream data integrated with machine learning re-optimization loops to compress the overage rate to under 20 percent. Transitioning to this automated predictive framework allows biopharmaceutical organizations to maintain a 99.9 percent service level while significantly mitigating clinical waste.
Macro-Level Constraints In Clinical Supply Planning
Clinical trial supply planning is mathematically more complex than commercial distribution due to its absolute dependency on stochastic, or probabilistic, variables. While commercial supply channels lean on long-term historical sales baselines, clinical logistics must react to real-time nonlinear inputs:
- Nonlinear patient enrollment: Clinical operations traditionally project recruitment using flat linear rates, such as 1.5 patients per site per month. Real-world data across global trials indicates that enrollment actually follows an asymmetrical S-curve characterized by prolonged initial lag phases and sharp, unpredictable regional surges.
- Protocol-driven variability: Dose titrations based on patient weight or biomarker toxicity, high participant dropout percentages, and sudden protocol amendments alter the demand curve mid-trial, rendering static precalculated inventory schedules obsolete.
- The randomization and blinding imperative: To prevent unblinding, supply planning algorithms must orchestrate drug distribution using complex interactive response technology (IRT) variables. Kits must be assigned and shipped without exposing treatment or control configurations to investigators or patients.
- Volatile stability and expiry windows: Investigational materials frequently operate with concurrent stability testing, meaning expiry windows are constantly updated. Managing this across hundreds of sites requires real-time algorithmic first-expiry, first-out (FEFO) enforcement.
Integrated Data Architectures
The core prerequisite of any predictive supply engine is the consolidation of siloed data streams. An optimal AI planning algorithm requires continuous API integration across four distinct software ecosystems:
- Interactive Response Technology (IRT/IxRS): Captures high-frequency transactional data at the point of care, including local kit counts, real-time patient randomization numbers, and upcoming scheduled visits.
- Clinical Trial Management Systems (CTMS): Supplies macro-level operational milestones, such as institutional country-level approvals, investigator site initiation dates, and historical regional enrollment metrics.
- Electronic Data Capture (EDC): Tracks patient-specific clinical inputs. By parsing blinded metrics like adverse event frequencies and early dose adjustments, predictive models can evaluate the probabilistic risk of localized dropouts.
- Enterprise Resource Planning (ERP): Provides supply-side baselines, monitoring current bulk drug substance or drug product quantities, packaging lead times, and global depot storage capacities.
Machine Learning Frameworks And Predictive Execution
Dynamic enrollment via XGBoost and LSTM networks
Rather than relying on historical averages, advanced predictive engines process historical data across tens of thousands of past protocols using gradient-boosted trees (XGBoost) and long short-term memory (LSTM) neural networks. LSTMs are uniquely capable of detecting time-series dependencies in patient enrollment across varying geolocations. By factoring in trial phase, therapeutic indication, protocol complexity (such as inclusion or exclusion criteria counts), and CRO performance benchmarks, the model runs thousands of Monte Carlo simulations. This shifts forecasting from a single fixed target to a fluid probability density function, defining localized demand with an accuracy rate exceeding 85 percent.
Dynamic drug pooling and variable safety stock formulas
In legacy logistics, a fixed safety stock buffer is assigned to every open site (for example, maintaining a constant baseline of 10 kits per location). For a trial spanning 100 sites, this traps 1,000 kits in the field.
AI-enabled networks utilize dynamic drug pooling. If multiple protocols use identical core formulations or dosages, the inventory is maintained as a shared, unallocated pool at regional hubs. The engine constantly calculates a variable safety stock (SSv) for each site using an optimized variant of the classic inventory formula:
SSv = Z × √(L · σd 2 + D2 · σL 2)
Where Z represents the standard normal distribution score corresponding to the desired service level (e.g., 99.9 percent stockout protection); L is the replenishment lead time from depot to site; σd 2 is the variance in real-time patient enrollment velocity calculated over rolling 14-day windows; D is the average demand velocity; and σL 2 is the variance in transport and customs clearance timelines.
When an individual site's enrollment velocity drops, its local safety stock requirement automatically contracts within the IRT system, and inventory is rerouted to high-velocity locations, suppressing overproduction.

Empirical Case Studies
Representative Scenario 1: Algorithmic waste reduction in adaptive Phase 3 oncology
A multicenter Phase 3 oncology trial involving 140 global sites presented a complex logistical challenge: the trial design featured three distinct titration pathways based on patient-specific biomarker expressions. An initial manual supply plan calculated that maintaining a 99.5 percent service level would require an overage rate of 65 percent, translating to millions of dollars in anticipated waste.
- The Action: The sponsor integrated an ML optimization tool directly with their live IRT system. The engine evaluated rolling seven-day enrollment trends and dynamically recalibrated site-specific shipment triggers via the variable safety stock matrix.
- The Result: The system executed the entire trial with zero patient stockouts while compressing total drug waste from the projected 65 percent to 14.2 percent. This optimization saved $5.1 million in drug manufacturing and cold chain shipping overhead.
Representative Scenario 2: Deep learning for portfolio-wide demand optimization
A major biopharmaceutical portfolio evaluation investigated the deployment of a fully convolutional network (FCN) trained on a multivariable data set tracking more than 100,000 active patient milestones across diverse therapeutic indications.
- The Action: The FCN model analyzed complex historical variables, including regional investigator site density, protocol inclusion stringency, and historical customs delay patterns, to predict the exact calendar month of trial completion.
- The Result: Aligning these deep learning enrollment timelines directly with master manufacturing schedules allowed the validation and scheduling teams to dynamically shift production slots. This prevented the premature packaging of short-dated biological drug products, yielding a 28 percent reduction in expired material write-offs across the entire pipeline.
Implementation Road Map And Operational Hurdle Management
Phase 1: Data cleansing, harmonization, and API alignment (months 1–4)
The immediate focus must center on data engineering. Centralized data architecture must be constructed using secure web APIs to feed data from disparate IRT, CTMS, and ERP databases into a consolidated data lake. The primary objective during this phase is to fully standardize data fields across all software layers, ensuring terms like “active site” or “validated container” maintain identical parameters across all departments.
Phase 2: Parallel run execution and hyperparameter calibration (months 5–8)
To validate the system safely, the predictive model must run in parallel with legacy spreadsheet workflows. The algorithm's short-term demand and enrollment forecasts are matched against actual real-world outcomes month over month. The core objective is to calibrate the model's hyperparameters (such as adjusting the weights of local CRO historical metrics) to achieve a predictive accuracy baseline of at least 85 percent before transitioning to active operational deployment.
Phase 3: Closed-loop automation and continuous optimization (months 9+)
Upon hitting accuracy thresholds, the predictive engine is given live execution clearance. The model automatically outputs optimized shipment sizes, batch allocations, and distribution routes directly to clinical supply managers, requiring only a single-click validation step.
Overcoming Core Operational Hurdles
- The GxP compliance and the black box barrier: Regulatory bodies (such as the FDA and EMA) operate under strict GMP and GCP mandates. Opaque black box deep learning models will fail quality assurance audits if their core rationale is untraceable. Organizations must deploy explainable AI (XAI) frameworks that output an audited, step-by-step mathematical trace explaining exactly why a specific inventory buffer or shipment size was selected.
- Planners' cultural change management: Technical teams often look at automated suggestions with skepticism. Change management programs must reframe the AI system not as an existential threat to human oversight but as an advanced navigation instrument that automates data aggregation so specialists can focus on complex vendor relationships, risk mitigation, and validation troubleshooting.
Future Horizons
The late 2020s are seeing an evolution past standard localized enrollment modeling. Advanced systems are beginning to leverage anonymized electronic health records during initial protocol architecture phases. By checking actual regional patient densities before a trial is initiated, logistics teams can configure regional depot structures with pinpoint accuracy.
Furthermore, integrating machine learning with live IoT sensory devices embedded in shipping containers enables multi-agent networks to calculate cold chain failure probabilities in transit. If an engine identifies an unseasonable temperature shift or a regional transit delay along a designated shipping lane, it automatically recalculates shipping vectors to guarantee biological product integrity.
About The Author:
 Shanker Ojha is a biopharmaceutical validation professional with over a decade of hands-on experience managing complex commissioning, qualification, and validation (CQV) cycles, QMS, and GMP compliance. His career is built on the shop floor, bridging the gap between technical engineering and time-sensitive manufacturing operations, including leading major process validation projects for biologics.
Shanker Ojha is a biopharmaceutical validation professional with over a decade of hands-on experience managing complex commissioning, qualification, and validation (CQV) cycles, QMS, and GMP compliance. His career is built on the shop floor, bridging the gap between technical engineering and time-sensitive manufacturing operations, including leading major process validation projects for biologics.
Having worked directly inside manufacturing hubs, Ojha knows firsthand how clinical supply lines stall when validation is treated as a retrospective paperwork drill. His focus is on synchronizing computer system validation (CSV) with physical assets and using risk-based frameworks to compress timelines. Shanker advocates for floor-level psychological safety, ensuring operators can flag technical anomalies instantly to resolve issues in real time.
References:
- Al-Hourani, S. & Weraikat, D. A systematic review of artificial intelligence (AI) and machine learning (ML) in pharmaceutical supply chain (PSC) resilience: current trends and future directions. Sustainability17, 6591 (2025).
- Boualam, M. et al. Toward a demand-driven supply chain: BLR evaluating the impact of AI and ML integration in the healthcare and pharmaceutical industry. MDPI Proceedings97, 2 (2025).
- Nuta, S. et al. Artificial intelligence in pharmaceutical supply chain management. Int. J. Sci. Technol.3, 7919-7928 (2025).
- Sadoon, E., Venkatadri, U. & Ghasemi, A. A conceptual framework for logistics management and project planning in the clinical trials industry. Logistics7, 88 (2023).
- Shoieb, A. A Machine Learning Approach for Predicting Clinical Trial Patient Enrollment in Drug Development Portfolio Demand Planning. (Univ. Tennessee, 2024).
- Attaran, M. The role of AI and digital twins in transforming pharmaceutical supply chains. J. Bus. Technol.12, 45-58 (2024).
- Bapat, A. & Taylor, M. Reducing overage in biologics clinical trials: a data-driven optimization approach. J. Clin. Logistics8, 112-125 (2023).
- Chen, X. & Wang, Y. Stochastic optimization models for dynamic drug pooling in international clinical trials. Eur. J. Oper. Res.315, 204-218 (2024).
- Garrison, K. & Patel, R. Integration of IRT and ERP systems: the foundation for real-time clinical supply visibility. 9. Pharm. Exec. Rep. 41, 34-39 (2025).
- Haddad, M. et al. Machine learning for patient enrollment forecasting in cold-chain dependent clinical protocols. Int. J. Prod. Econ. 268, 109-122 (2024).
- Ivanov, D. Digital twin-driven pharmaceutical supply chains: resilience and sustainability analysis. Int. J. Logistics Res. Appl.26, 412-431 (2023).
- Kumar, A. & Suresh, N. Explainable AI (XAI) frameworks for GxP compliance in pharmaceutical logistics. Regul. Aff. J.19, 77-89 (2025).
- Lopez, S. & Martinez, J. Application of long short-term memory (LSTM) networks to clinical trial enrollment forecasting. Bioinformatics Bioprocess Eng.11, 301-314 (2024).
- Mehra, R. & Das, G. Optimization of variable safety stock in biopharmaceutical supply networks under high uncertainty. Oper. Res. Health Care15, 88-101 (2025).
- Olegario, P. Interactive Response Technology (IRT) as a driver for dynamic inventory routing in clinical trials. J. Pharm. Sci.112, 2135-2147 (2023).
- Ramos, M. et al. Predictive analytics in cold-chain logistics: preventing biological degradation in transit. Vaccine Biologics Logistics7, 14-26 (2024).
- Smith, J. A. & Davis, L. E. Quantifying waste in precision medicine clinical trials: an industry-wide benchmark study. Ther. Innovation Regulatory Sci.58, 445-456 (2024).
- Thomas, L. & Wickramasinghe, N. Utilizing real-world data (RWD) for predictive clinical supply network design. Int. J. Med. Inform. 182, 105-118 (2025).
- Vogel, F. & Ziegler, H. Multi-agent systems for automated expiry management in global depot networks. Comput. Ind. Eng. 189, 109-124 (2024).
- Zhao, Q. & Zhou, K. Gradient-boosted decision trees (XGBoost) for modeling enrollment variance in phase III protocols. J. Biopharm. Stat. 33, 612-627 (2023).