
Clinical Pharmacy-Led Perspective On Clinical Trial Supply Innovation
By Marija Tubic Grozdanis, Ph.D., clinical pharmacist, Johannes Gutenberg University Medical Center

Trained pharmacy personnel ensure that the investigational medicinal product (IMP) for clinical trials is appropriate for use and is handled and stored safely and correctly.
Clinical pharmacists work directly with patients, site personnel, and sponsor systems to ensure IMP handling, dispensing, and accountability processes remain aligned with protocol-defined clinical supply strategies. Within clinical trial supply systems, they act as execution nodes between sponsor-defined supply strategies and real-world dispensing environments, ensuring protocol-compliant IMP availability at the point of use.

Image by University Medical Centre Mainz
Enrollment dynamics directly influence clinical supply forecasting, depot sizing, and resupply frequency, making patient recruitment variability a critical input into supply chain planning models. From a supply perspective, enrollment assumptions directly drive demand forecasting, resupply frequency, and depot sizing strategies. Most enrollment projections in clinical trials are based on best-case scenarios, even though patients may hesitate to participate due to limited understanding of the benefits of clinical research, general distrust of the research process, or competing priorities. Clinical pharmacists can support identification and education of eligible participants and reduce enrollment-driven supply variability by improving predictability of patient demand curves at the site level.
To ensure that every patient receives the right treatment at the right time in a clinical trial, clinical pharmacy contributes to the development and implementation of patient-centric, decentralized, and automated clinical trial supply systems.
Adaptive Trial Design And Clinical Supply Execution
Adaptive platform trials can test multiple therapies, adjust sample sizes, discontinue ineffective treatment arms, or modify dosing during the trial. This approach allows sponsors to adapt the trial design while the trial is still ongoing.
In adaptive trials, clinical supply systems must operate under dynamic demand conditions, driven by protocol changes, cohort expansion, and treatment arm adaption, requiring flexible packaging strategies, late-stage randomization binding, and responsive resupply logic. it is essential to develop, validate, and implement efficient supply management systems that provide just-in-time supply. Clinical pharmacy can support various packaging strategies with validated workflows to ensure repeatability and GMP compliance, allowing delayed commitment of manufactured product and comparator (e.g., placebo) to a dosing regimen or protocol as late as possible in the supply chain process.
Images by University Medical Centre Mainz
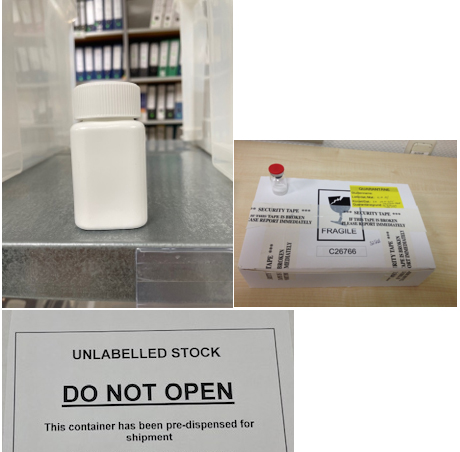
There are several ways in which labeling can be used to maximize the flexibility of clinical supplies. Sponsors deliver the unlabeled primary packaged material (brite stock) and pre-generated, approved labels for country, dose level, and treatment group to the clinical pharmacy. At the point of trigger (randomization, cohort escalation, or amendment activation), the pharmacy executes label activation and kit assembly under controlled GMP-aligned conditions. This creates a defined operational decision point in the supply chain where treatment assignment is implemented at the pharmacy layer rather than during manufacturing or central packaging. The pharmacy can act as a central depot, delivering a pre-labeled pool of product to the sites. Additional kits are labeled on demand to ensure sufficient supply throughout the trial.
Decentralized Clinical Trials: When A Dispensing Order Becomes A Shipment Order
A decentralized approach enables remote patient participation, reducing the need for frequent site visits and improving accessibility and efficiency. In most EU-member states, approval for this approach can be obtained on a case-by-case basis following regulatory discussion. Sponsors must provide evidence that decentralized elements contribute to patient safety and improve access to therapy.
The most commonly used model for direct-to-participant IMP supply in clinical trials is the one with the fewest regulatory barriers, in which the IMP is shipped from the investigative site or central pharmacy to the participant´s home or local pharmacy. This effectively transforms dispensing events into controlled logistics transactions, requiring integration between pharmacy systems, couriers, temperature monitoring technologies, and chain-of-custody documentation. This shift requires tight synchronization between IRT/RTSM systems, courier tracking, and temperature excursion monitoring to maintain chain-of-custody integrity.
Is The IMP Stored And Handled Properly At The Patient’s Home?
Health authorities require that the Quality-Investigational Medicinal Product Dossier (Q-IMPD) includes all detailed information on how the drug is prepared, handled, and administered. However, post-manufacturing handling by caregivers and patients is less clearly defined in regulatory guidance and is often inconsistent.
A significant challenge is ensuring temperature-controlled storage outside clinical sites, where continuous environmental monitoring and excursion management systems are typically not available.
The EU-funded RealHOPE project investigated how protein drugs are handled throughout their life cycle (https://realhope.se) and developed tools and methods to measure specific stressors in real-world handling. Few published studies provide information on the environmental conditions to which protein medicines are exposed during normal use.1,2,3
Given the complexity of handling protein-based biological drugs, closer collaboration is needed among pharmaceutical developers, pharmacists, healthcare providers, device manufacturers, public researchers, and patients to reduce variability in real-world exposure conditions that directly impact product integrity within decentralized supply models.
The Future Of Clinical Trial Supply: Patient-Centric, Decentralized, And Smart
Clinical trial supply strategies must balance patient needs and lifestyles with patient satisfaction and safety.

Image by University Medical Centre Mainz
These trends increasingly require supply chains capable of small-batch, high-variability, and near-patient manufacturing and distribution models rather than centralized large-scale batch release systems.

3D Printing As A Novel Manufacturing Approach
3D printing platforms enable resilient, decentralized, and patient-centric pharmaceutical production. Smart manufacturing brings production closer to the patient and enables rapid, flexible, GMP-compliant small-scale production of investigational medicines directly supporting supply chain decentralization and kit customization.
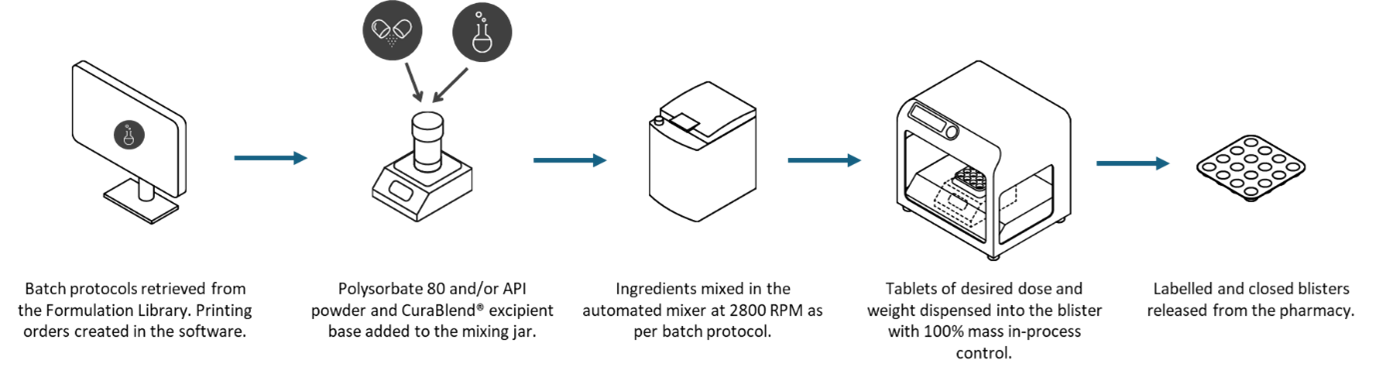
Overview of the non-sterile compounding workflow in a compounding system solution (CSS)
Potential Of 3D Printing In Clinical Trial Supply
- Easy blinding and placebo creation
- Rapid dose adjustment
- Customizable shapes, sizes, and sensory characteristics
- Small batches with diverse formulations (tablets, capsules, films, minitablets, suppositories, controlled-release systems, polypills
- Reduced development time and costs
- On-demand printing and reduced supply chain dependency
- Sustainable processes with less waste and faster delivery


Image by University Medical Centre Mainz
Challenge And Opportunities In Pediatric And Special-Population Trials
Children often have limited access to innovative treatments due to a lack of pediatric-specific safety data and regulatory authorization. Early-phase pediatric trials introduce high variability in dose requirements and formulation needs, which directly impacts clinical supply planning assumptions, packaging flexibility, and kit configuration strategies.
The innovative therapy options include new drugs administered orally, such as tablets and capsules. Oral therapies allow children to remain in their family environment, improving psychosocial well-being.
Hospital pharmacies can compound individualized capsules or suspensions in the calculated dosage for pediatric patients, but manual compounding is time-consuming, difficult to scale, and lacks industrial-level quality assurance. Compounded preparations do not undergo the same rigorous controls as approved medicinal products, increasing the risk of variability in drug concentration and performance.
There is an urgent need for child-friendly, age-appropriate, targeted therapies to improve outcomes and reduce treatment-related harm in pediatric patients. Regulatory agencies also strongly encourage the development of innovative oral formulations suitable for pediatric and special-population dosing requirements.
The same technology can support patients suffering from metabolic disorders where patient-specific dose adjustment is required and further investigation is needed or to produce gender-specific formulations based on individual pharmacokinetic profiles. Another application is the combination of multiple therapies in a single dosage form, reducing the burden of polypharmacy and the risk of errors and toxicity. However, implementation of this technique faces many challenges, such as the absence of regulatory frameworks and synchronization with new point-of-care manufacturing guidelines.
Conclusion
The future of clinical trial supply is patient-centric, decentralized, and driven by smart manufacturing in precise, flexible small batches. Clinical pharmacy welcomes and supports the implementation of innovative manufacturing approaches – including decentralized and bedside production – bringing greater automation, flexibility, agility, and sustainability to clinical trial supply while ensuring patient safety, trial success, and compliance with international quality standards.
References:
- Cappelletto E, Kwok SC, Sorret L, Fuentes N, Medina AM, Burleigh S, Fast J, Mackenzie IS, Fureby AM, Paulsson M, Wahlgren M, Elofsson U, Flynn A, Miolo G, Nyström L, De Laureto PP, De Paoli G. Impact of Post Manufacturing Handling of Protein-Based Biologic Drugs on Product Quality and User Centricity. J Pharm Sci. 2024 Aug;113(8):2055-2064.
- Franzese C, Hawthorne J, Katsaros D, Coyne M. Patient Experience and Improvement Opportunities in Self-Administered, Large-Volume Subcutaneous Infusion at Home. Patient Prefer Adherence 2025 Aug;19:2459-2491
- Charlotte Sikking, T.Ton Dinh, Mirjam Crul, Stefan G. Romeijn, Charlotte van Kesteren, Marieke M. Beex-Oosterhuis,. Analysis of the formation of (sub)visual particles in ready-to-administer trastuzumab infusion bags during transport from the hospital pharmacy to patients at home. J of Pharm Sci 2026;115(3): 104164
About The Author:
 Marija Tubic Grozdanis, Ph.D., is a clinical pharmacist at Johannes Gutenberg University Medical Center in Mainz, Germany. With a background in pharmaceutical technology, her early research focused on delayed-release dosage forms and gastrointestinal simulation to understand drug absorption. Since 2008, she has served as lead pharmacist for clinical trials and qualified person, managing a team supporting studies across all phases and therapeutic areas. Her current work centers on personalized medicine, including automated compounding and integration into healthcare under evolving regulatory frameworks. She collaborates across disciplines, notably with a children’s hospital on 3D-printed pediatric medicines. She is active in GERPAC and c4c expert groups and has lectured in clinical pharmacokinetics since 2023.
Marija Tubic Grozdanis, Ph.D., is a clinical pharmacist at Johannes Gutenberg University Medical Center in Mainz, Germany. With a background in pharmaceutical technology, her early research focused on delayed-release dosage forms and gastrointestinal simulation to understand drug absorption. Since 2008, she has served as lead pharmacist for clinical trials and qualified person, managing a team supporting studies across all phases and therapeutic areas. Her current work centers on personalized medicine, including automated compounding and integration into healthcare under evolving regulatory frameworks. She collaborates across disciplines, notably with a children’s hospital on 3D-printed pediatric medicines. She is active in GERPAC and c4c expert groups and has lectured in clinical pharmacokinetics since 2023.